| PYQ Relevance: Mains: Q Analyse the salience of ‘sect’ in Indian society vis-a-vis caste, region, and religion.(UPSC IAS/2022) Q Discuss the main objectives of Population Education and point out the measures to achieve them in India in detail. (UPSC IAS/2021) Q “Empowering women is the key to controlling the population growth.” Discuss. (UPSC IAS/2019) Prelims: India is regarded as a country With a “Demographic Dividend” This is due to (UPSC IAS/2011) (a) Its high population in the age group below 15 years (b) Its high population in the age group of 15-64 years (c) Its high population in the age group above 65 years (d) Its high total population |
Note4Students:
Prelims: Population Trends; Minorities;
Mains: Society; Minorities; Religious demography; Effects of Policies and Programs on Demographics;
Mentor comment: The recent report ‘Share of Religious Minorities: A Cross-Country Analysis (1950-2015)’ conducted by the Economic Advisory Council analyzes the demographic changes in the religious composition of Indian Society as well as across 167 countries from 1950 to 2015. It focuses on the shifting shares of majority and minority religious groups, highlighting trends such as the decline in the Hindu population and the growth of the Muslim population in India. The study emphasizes the importance of understanding these changes as indicators of relative well-being within a country. We need to study this analysis as it is based on the premise that any change in minority populations is influenced by policies related to defining and treating minorities in our country.
Let’s learn
_
Why in the News?
The recent working paper titled ‘Share of Religious Minorities: A Cross-Country Analysis (1950-2015)’ by the Economic Advisory Council to the Prime Minister (EAC-PM), has major observations on Indian religious demographics.
| Key highlights made by EAC-PM Report: The paper is based on the baseline year as 1950, because this was the time around when the International Human Rights Framework was introduced under the aegis of the newly created United Nations. Considering the global trends of declining majority, India too has witnessed a reduction in the share of the majority religious denomination by 7.82%. According to the Report, the Hindu population decreased by 7.82% (1950-2015), while that of Muslims increased by 43.15%, suggesting a conducive environment in the country to foster diversity. The share of the Christian population rose from 2.24% to 2.36% — an increase of 5.38% between 1950 and 2015. While the share of the Sikh population increased from 1.24% in 1950 to 1.85% in 2015 — a 6.58% rise in their share, the share of the Parsi population in India witnessed a stark 85% decline, reducing from 0.03% share in 1950 to 0.004% in 2015. South Asian Trends: Within the neighborhood, the share of the majority religious denomination has increased and minority populations have shrunk alarmingly across countries like Bangladesh, Pakistan, Sri Lanka, Bhutan, and Afghanistan. Minority populations from across the neighborhood come to India during times of duress. 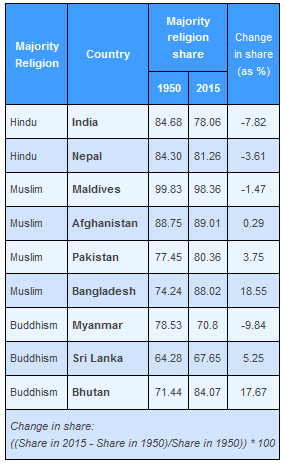 |
The present controversy over the EAC-PM Report:
- The PM-EAC report on religious minorities in India has sparked debate due to its timing, outdated data, and selective focus.
- For example, firstly, it does not highlight the nearly 1,520% increase in share in the total population of Buddhists, for every one Muslim, five Hindus were born during this period.
- Secondly, the Hindu population has tripled, and the Total Fertility Rate (TFR) of Muslim women saw a drop of 2.05 against Hindu women’s TFR by 1.36, making it controversial.
- Despite concerns raised by some, the demographers do not see that the Hindus are losing their majority status, given the historical context and current demographic patterns.
- For example, when Hindus could retain their majority status during the 800 years of so-called Mughal rule, they cannot be in danger today.
Present rhetoric and challenges:
- Need to have a broader outlook: Focusing solely on Total Fertility Rates to assess a group’s status overlooks broader factors like education and socioeconomic conditions.
- Need to survey Public Participation: The representation of a particular religious group in the state’s power structure is a crucial indicator of its well-being.
- The Finance Minister recently highlighted the growth of the Muslim population as a positive sign, emphasizing that Indian Muslims enjoy more rights compared to minorities in some Muslim-majority countries.
- India is set to become the country with the largest Hindu and Muslim populations by 2050, showcasing the diversity and coexistence within the nation.
What does the Population Data say?
- Stabilizing of the Minorities: The data on the decline in Muslim women’s fertility rates, as seen in Census data, indicates a positive trend toward stabilization. (according to the United Nations Population Fund)
- Demographers predict that by the end of the century, Muslims may constitute around 18.8% of India’s population, with Hindus maintaining a significant majority at 74.7%.
- Regional Variations: Various states have already achieved fertility rates below replacement levels, signaling a broader trend of population stabilization.
- While the Population Regulation Bill in 2019 or the Population (Control) Bill in 2021 has been introduced, some demographers generally emphasize the importance of addressing population dynamics through education, healthcare, and socioeconomic development.
- Lack of Data-evidences: Claims of alarming Muslim population growth in certain regions like Assam lack substantial evidence, with data showing different growth patterns across states.
- Illegal Muslim infiltration from Bangladesh is generally said to be responsible for the demographic change since the 1970s in Assam.
Are Coercive Methods Counter-productive?
- International Norms and the Indian Government stance: Being a signatory to international covenants such as the International Covenant on Civil and Political Rights (ICCPR), India has to abide by the international norms on population control.
- The United Nations Human Rights Committee has categorically mandated that state parties to ICCPR cannot adopt policies that are compulsory, coercive, or discriminatory.
- Even the National Population Policy, of 2000 focused on more relevant socio-cultural factors such as age at marriage, age at birth, girl education, maternal and child health, and voluntary and informed consent over coercive methods.
Conclusion: To address concerns about population growth, efforts should concentrate on improving education and economic opportunities for all communities, including Muslims, rather than resorting to coercive measures.






![[8 April 2024] The Hindu Op-ed: Shaping India’s path to inclusive Health Care](https://d18x2uyjeekruj.cloudfront.net/wp-content/uploads/2024/04/WhatsApp-Image-2024-04-09-at-6.33.17-PM-1568x882.jpeg)