On Tuesday, June 18, the Marriage Equality Billwas approved by the Thai Senate, the upper house of Thailand’s National Assembly, with overwhelming support.
What does the Bill entail?
Gender-Neutral Language: The bill replaces gender-specific terms such as “husbands” and “wives” in Thai marriage laws with gender-neutral terms like “spouse” and “person”. This change allows any two individuals, regardless of their gender, to marry each other.
Equal Rights: Same-sex couples will have the same rights as heterosexual couples in various legal and practical aspects, including:
Adoption rights: Same-sex couples can adopt children.
Inheritance rights: They are entitled to inherit property from their spouses.
Tax benefits: They will receive similar tax benefits as heterosexual married couples.
Legal decision-making: They can make legal decisions on behalf of their spouses, such as consenting to medical treatment.
Recognition and Protection: The bill ensures that same-sex marriages are legally recognised and protected, providing stability and legal security to LGBTQ+ couples in Thailand.
Public Support: The bill’s passage reflects growing societal acceptance and support for LGBTQ+ rights in Thailand. Public opinion has been largely positive, with significant cross-party support in the Thai Senate and lower house of the National Assembly.
What about other Asian countries?
Criminalization: Many Asian countries, beyond those mentioned (Thailand, Taiwan, Nepal), still criminalize same-sex sexual activity. This includes countries like Malaysia, Myanmar, Pakistan, and Sri Lanka, where laws derived from colonial-era penal codes often penalize homosexuality with imprisonment or fines.
Lack of Legal Recognition: Most Asian nations do not legally recognizesame-sex marriages or partnerships.
Even in countries where same-sex relations are not explicitly criminalized, there is often no legal framework for marriage or civil unions for LGBTQ+ individuals.
Legal Battles: In countries like India, legal battles continue as activists seek to overturn discriminatory laws and secure legal recognition for same-sex relationships, including marriage.
International Pressure: International human rights organizations and diplomatic efforts sometimes exert pressure on Asian governments to improve LGBTQ+ rights. However, progress is often slow and faces strong domestic resistance.
Note: Currently, same-sex marriage is legal in 36 countries (not including Thailand) globally, according to LGBTQ+ rights advocacy Human Rights Campaign.
Way forward:
Legal Challenges and Reform: Support ongoing legal challenges in courts across Asia to overturn discriminatory laws and promote legal recognition of same-sex relationships. This includes advocating for legislative reforms that protect LGBTQ+ rights, including the recognition of same-sex marriages or civil unions.
International Pressure and Diplomacy: Encourage international human rights bodies, governments, and diplomatic missions to engage with Asian countries diplomatically, urging them to uphold international human rights standards, including LGBTQ+ rights.
The phenomenon of ageing stands out as one of the most significant developments of this century, characterized by notable advancements in human longevity alongside historically low reproduction rates.
About the Magnitude and Multiplication of the aged population
The magnitude of Aging Population: The 21st century is witnessing a significant demographic shift marked by a notable increase in human longevity.
Improved healthcare and living conditions have contributed to a rise in life expectancy, leading to a larger elderly population. By mid-century, India is projected to have around 319 million elderly people, growing at a rate of approximately 3% annually.
Multiplication of Aging Phenomenon: Despite longevity gains, there is a simultaneous decline in fertility rates, leading to an ageing population with a lower proportion of younger generations.
This demographic shift poses challenges related to healthcare, social security, and economic sustainability. The elderly population is becoming increasingly feminized, with a higher prevalence of elderly women due to longer life expectancy and higher widowhood rates.
Aged Population as per the 2011 Census:
According to the 2011 Census of India, the population of people aged 60 and older in India was 104 million, which is 8.6% of the total population. This is an increase from 5.6% in 1961.
The census also found that 53 million of the elderly population were female and 51 million were male, with a sex ratio of 1033. 71% of the elderly population lived in rural areas and 29% lived in urban areas. Additionally, 5.18% of the elderly population, or 53,76,619 people, had some disability
Issues and Challenges
Vulnerabilities of the Elderly: Many elderly individuals in India face significant vulnerabilities, including limitations in activities of daily living (ADL), multi-morbidity, poverty, and lack of financial security.
A substantial proportion of the elderly report poor health conditions, with a high prevalence of chronic diseases such as diabetes and cancer.
Mental health issues, particularly depression, are also prevalent among the elderly population.
Social and Economic Insecurities: Food insecurity affects a notable percentage of the elderly, with reports of reduced portions or skipped meals due to economic constraints.
Lack of legal protection: Awareness and access to welfare measures and legal protections for the elderly are low, with limited knowledge about schemes like IGNOAPS, IGNWPS, and Annapurna.
Abuse and Neglect: Elder abuse is a significant concern, especially for elderly women in rural areas who often experience neglect and mistreatment within their families and communities.
Social exclusion and limited opportunities for productive engagement exacerbate feelings of insecurity and marginalization among the elderly.
Way Forward:
Enhancing Social Support and Welfare Measures: Strengthening awareness and accessibility of welfare schemes and legal protections for the elderly. Implementing social security measures to ensure financial stability and improve quality of life for ageing populations.
Healthcare and Mental Well-being: Prioritizing healthcare interventions tailored to the needs of the elderly, including preventive measures against chronic diseases and mental health support. Promoting healthy ageing through lifestyle interventions and healthcare policies that address the unique challenges of an ageing population.
Empowerment and Social Inclusion: Fostering social inclusion through community engagement and initiatives that empower the elderly to contribute actively to society. Developing innovative institutional frameworks that value the elderly as assets and promote their participation in societal development.
Mains PYQ:
Q. Critically examine the effects of globalization on the aged population in India. (UPSC IAS/2013)
Q Discuss the possible factors that inhibit India from enacting for its citizen a uniform civil code as provided for in the Directive Principles of State Policy. (UPSC IAS/2015)
Q Customs and traditions suppress reason leading to obscurantism. Do you agree? (UPSC IAS/2020)
Mentor comment: Interfaith marriages in India face legal and societal challenges despite protections under the Special Marriage Act, 1954. Recent judicial interventions have raised concerns about misinterpretations, impacting couples’ rights to choose partners freely. Such marriages often encounter opposition from families and communities, leading to social tensions. Efforts to protect couples through legal frameworks are crucial amid ongoing debates on religious and cultural sensitivities.
Let’s learn!
Why in the News?
A recent order from the Madhya Pradesh High Court has raised concerns about the interpretation of the law regarding inter-faith marriages and the scope of the Special Marriage Act, 1954.
About Special Marriage Act, 1954:
•The SMA was passed by the Parliament on October 9, 1954. •It governs a civil marriage where the state sanctions the marriage rather than the religion. •The minimum age to get married under the SMA is 21 years for males and 18 years for females. Need for SMA: •Issues of personal law such as marriage, divorce, and adoption are governed by religious laws that are codified. •These laws, such as the Muslim Marriage Act,1954, and the Hindu Marriage Act, 1955, require either spouse to convert to the religion of the other before marriage. •However, the SMA enables marriage between inter-faith or inter-caste couples without them giving up their religious identity or resorting to conversion.
Erroneous Considerations
Typical Assessment Under Article 226: When a petition for police protection is filed under Article 226 of the Constitution, the High Court usually assesses the violation of the petitioners’ rights and the threat they face.
Extended Protection Examples:
The Madras High Court granted protection to a lesbian couple, recognizing the dangers they faced.
The Punjab and Haryana High Court provided protection to a live-in couple, emphasizing the protection of their fundamental rights under Article 21 of the Constitution.
Contrasting Focus of Madhya Pradesh HC: Instead of focusing on the threats faced by the couple, the HC focused on the validity of the couple’s impending marriage, disregarding their right to life and liberty.
What is Article 226 of the Constitution?: Article 226 grants the High Courts of Indian states the power to issue writs. These writs are primarily meant for the enforcement of fundamental rights guaranteed under Part III of the Constitution or for any other legal purpose. The High Courts have the authority to issue writs such as habeas corpus, mandamus, prohibition, quo warranto, and certiorari.
Dilution of the Special Marriage Act
Contradictory Order: The Madhya Pradesh High Court’s order contradicts the core principles of the Special Marriage Act.
Irrelevant Supreme Court Precedent: The court erroneously relied on a Supreme Court precedent related to property succession under Mohammedan Laws, which is irrelevant to the validity of inter-faith marriages under the Special Marriage Act.
Misinterpretation of Section 4: The court misinterpreted Section 4 of the Act, which excludes marriages between close relatives, not inter-faith marriages.
Act’s Purpose: The Act is designed to facilitate marriage between any two Indian nationals, regardless of their faith.
Present status of Special Marriages:
Significance of the Order: The Madhya Pradesh High Court order is significant given the current social and political climate, where inter-faith and inter-caste marriages face vigilantism and right-wing propaganda.
Ongoing Petitions: There are ongoing petitions challenging unconstitutional provisions within the Special Marriage Act, such as the prior notice requirement, pending before the Supreme Court.
Supreme Court’s Ruling in Shafin Jahan Case:
Emphasized the protection of personal liberty and the right to choose a life partner, regardless of faith or caste.
Justice D.Y. Chandrachud’s judgment highlighted that intimate personal decisions do not require social approval and are protected by the Constitution.
Way forward
Disregard of Shafin Jahan Judgment: The Madhya Pradesh High Court’s order disregards the spirit of the Shafin Jahan judgment, which prioritizes individual autonomy, privacy, and liberty.
Courts’ Responsibility: Constitutional courts must remember that jurisprudence favours autonomy and personal liberty.
While global gender parity has improved to 68.5% in 2024 from 68.4% in 2023, progress remains slow. The World Economic Forum’s report indicates it will take 134 years to achieve full parity at this rate.
The Global Gender Gap Report 2024
It is released by the World Economic Forum (WEF), and highlights significant disparities in gender parity across various sectors.
Present Scenario:
Global Gender Gap Report 2024:
The global gender gap stands at 68.5% closed, indicating slow progress towards gender parity.
Iceland leads with over 90% closure, while India has slipped to 129th position out of 146 countries, with 64.1% closure.
India’s slight regression is attributed to declines in education and political empowerment indices.
Challenges in India:
Despite improvements in economic participation, India needs to bridge gaps in education and political representation.
The labour force participation rate for women is 45.9%, indicating significant untapped potential.
Gender disparity in literacy rates persists, with women lagging 17.2 percentage points behind men, impacting India’s global ranking.
Significance of Low Gender Gap in the Education Sector:
Bridging the gender gap in education is crucial for enhancing women’s economic opportunities.
Measures such as preventing dropout rates among girls, imparting job skills, and ensuring workplace safety are essential.
Improving literacy rates and educational attainment levels for women can lead to higher economic productivity and empowerment.
Significance of Low Gender Gap in Political Representation:
India shows low representation of women in political bodies despite some progress. Women constitute only 13.6% of the Lok Sabha members, reflecting inadequate political empowerment.
Implementation of the Women’s Reservation Bill, aimed at reserving one-third of seats in legislative bodies, remains crucial for enhancing women’s political participation and influence.
Way forward:
Enhancing Education Access and Quality: Implement targeted policies to reduce the gender gap in education, focusing on increasing girls’ enrollment and retention rates.
Promoting Women’s Political Empowerment: Implement initiatives to encourage women’s active participation in politics, such as leadership training programs, awareness campaigns, and support networks.
Mains PYQ:
Q Can the vicious cycle of gender inequality, poverty and malnutrition be broken through microfinancing of women SHGs? Explain with examples. (UPSC IAS/2021)
FOGSI launched a detailed immunization plan for women in Mumbai, featuring essential vaccines and recommended dosages, presented by women’s health advocate Kajal Aggarwal.
About the Federation of Obstetric and Gynaecological Societies of India (FOGSI)
The Federation of Obstetric and Gynaecological Societies of India (FOGSI) is a prominent professional organization dedicated to advancing the field of obstetrics and gynaecology in India.
Foundation and Scope: FOGSI was established in 1950 and currently represents over 34,000 obstetricians and gynaecologists across India. It serves as a unified platform for healthcare professionals specializing in women’s health.
Objectives: The primary objective of FOGSI is to promote the study and practice of obstetrics and gynaecology through education, research, and advocacy. It aims to improve the standards of healthcare delivery for women in India.
Significance of Preventive Health Care
Early Detection and Intervention: Preventive healthcare emphasizes regular screenings, vaccinations, and health checks to detect potential health issues early. This proactive approach allows healthcare providers to intervene early, often before symptoms appear, which can lead to better treatment outcomes and lower healthcare costs.
Promotion of Health and Well-being: By focusing on preventive measures such as healthy lifestyle choices, vaccination against preventable diseases, and routine health screenings, individuals can maintain optimal health and well-being. Preventive healthcare encourages behaviours that reduce the risk of chronic illnesses and promote longevity.
Reduction of Healthcare Burden: Investing in preventive healthcare can alleviate the burden on healthcare systems by reducing the prevalence and severity of diseases. By preventing illnesses before they occur or progress, fewer resources are needed for acute care, hospitalizations, and long-term management of chronic conditions.
Accessing ‘Vulnerable Period’
Postpartum Period: The postpartum period, typically defined as the first six weeks after childbirth, is a critical vulnerable period for women. During this time, the body undergoes significant physiological changes, including hormonal fluctuations and potential immune system alterations. These changes can increase susceptibility to infections and other health complications, necessitating close monitoring and appropriate medical interventions.
Menopausal Transition: Menopause marks a significant transition in a woman’s life when reproductive hormone levels decline, leading to various physical and psychological changes. This period can be accompanied by symptoms such as hot flashes, mood swings, and changes in bone density. Due to these changes, women may be more vulnerable to conditions like osteoporosis and cardiovascular disease.
Chronic Illness Management: Women with chronic conditions such as diabetes, hypertension, or autoimmune disorders may experience periods of vulnerability related to their specific health challenges. Fluctuations in hormone levels, stress, and lifestyle factors can exacerbate these conditions or increase the risk of complications. Healthcare strategies during these vulnerable periods often include personalized treatment plans, regular monitoring, and patient education to optimize disease management and promote overall well-being.
Conclusion: FOGSI’s launch of a women’s immunization schedule underscores their commitment to advancing women’s health through proactive care, addressing vulnerable periods like postpartum and menopause, and promoting disease prevention and management strategies.
Mains PYQ:
Q In order to enhance the prospects of social development, sound and adequate health care policies are needed particularly in the fields of geriatric and maternal health care. Discuss. (UPSC IAS/2020).
This year’s theme for International Fatty Liver Day, an awareness initiative observed annually in June, is ‘Act Now, Screen Today’. This theme holds more urgency now than ever before.
Liver Diseases in recent times
Liver diseases have long been primarily linked to excessive alcohol consumption, which continues to be a major cause of advanced chronic liver disease.
However, in recent years, a new and quietly escalating threat to liver health has emerged: non-alcoholic fatty liver disease.
India’s Growing Burden of Fatty Liver Disease
Note: MASLD, or Metabolic dysfunction-associated steatotic liver disease, is a reclassification of what was previously known as non-alcoholic fatty liver disease (NAFLD).
High Prevalence Rates: The global prevalence of Metabolic dysfunction-associated steatotic liver disease (MASLD) is estimated at 25-30%. In India, a 2022 meta-analysis revealed that the pooled prevalence of fatty liver among adults was 38.6%. Among obese children in India, the prevalence was around 36%.
Progression of Disease: The continuous damage caused by fatty liver leads to more severe conditions such as steatohepatitis and cirrhosis, often requiring liver transplants.
Causes of Growing Burden of Fatty Liver Disease
Lack of Early Detection: Fatty liver disease often goes undetected in early stages due to lack of symptoms. Diagnosis usually occurs at an advanced stage, when significant liver damage has already taken place.
Diet and Insulin Resistance: Excessive consumption of carbohydrates, especially refined carbs and sugars, leads to metabolic problems. High carbohydrate intake results in persistently high insulin levels and insulin resistance, promoting the conversion of excess glucose into fatty acids, which are then stored in the liver.
Initiatives Taken by the Government
Integration with NPCDCS: The Ministry of Health & Family Welfare launched operational guidelines for integrating NAFLD with the National Programme for Prevention & Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) in February 2021.
Health Promotion and Prevention: The Ayushman Bharat- Health and Wellness Centres (AB-HWCs) are being used to promote healthy living and screen for hypertension, diabetes, and other common NCDs.
Personalization is the Key
Tailored Screening Tests: The selection of screening tests and their frequency should be based on individual risk factors, including family history, lifestyle, and pre-existing health conditions.
Avoiding Generic Assumptions: Clinicians should not rely solely on age or physical markers; instead, they should consider a comprehensive risk profile. Non-communicable diseases are increasingly affecting diverse populations, including children.
Integrated Health Strategies: Combining dietary modifications, regular physical activity, and effective weight management to mitigate liver disease risks.
Frequent Screenings: Regular monitoring of liver health through non-invasive tools like vibration-controlled transient elastography. Continuous assessment of liver stiffness to detect early stages of liver fibrosis and monitor treatment responses.
Active Health Management: Emphasis on the importance of individuals taking control of their health by being aware of their diet and lifestyle choices.Encouragement of frequent health screenings to detect and manage liver disease early.
Way Forward:
Awareness Campaigns: Government initiatives focus on raising awareness about the importance of liver health and the risks associated with MASLD.
Health Screenings: Programs promoting comprehensive health screenings that include physical examinations, blood tests, and abdomen ultrasounds to detect liver diseases early.
Mains PYQ
Q The public health system has limitations in providing universal health coverage. Do you think that the private sector can help in bridging the gap? What other viable alternatives do you suggest? (UPSC IAS/2015)
India’s new cabinet has only 2 women ministers, down from 10 previously. The Global Gender Gap Report 2024 (by the World Economic Forum) ranks India third-lowest in South Asia, highlighting significant gender disparity in leadership and representation.
Comparison of Indian Ranking with Other Countries:
Global Gender Gap Report 2024: India ranked 129th out of 146 economies in the overall gender gap index. Ranked third-lowest among South Asian economies, behind Bangladesh, Nepal, Sri Lanka, and Bhutan.
Key points as Gender Gap Report 2024:
Economic Participation and Opportunity: 142nd, Health and Survival: 142nd, Educational Attainment: 112th, and Political Empowerment: Best rank (65th), but overall political representation remains low.
Political Empowerment: India performs relatively better on the head-of-state indicator (40.7%). However, women’s representation in ministerial positions (6.9%) and parliament (17.2%) is significantly lower. The region of South Asia shows high political disparity, with Nepal leading in ministerial representation (23.5%).
Educational Attainment: Despite high enrollment rates in primary, secondary, and tertiary education for women, the gap in literacy rate between men and women is significant (17.2 percentage points). India ranks 112th globally in this indicator.
Economic Participation: India has seen improvement in economic participation and opportunity, although it still ranks low (142nd). Challenges remain in bridging gender gaps in earned income, leadership roles, labour force participation, and technical professions.
Major observations around the causes of the Gender Gap
Patriarchal Structures: Patriarchy influences decision-making processes and power dynamics, often marginalising women’s voices and restricting their participation in political, economic, and social spheres.
Gender Bias: Gender bias manifests in various forms, affecting women’s access to resources, healthcare, education, and career advancement opportunities compared to men.
Gender Pay Gap: Women in India typically earn less than men for similar work, reflecting systemic inequalities in pay and compensation.
Occupational Segregation: Women are often concentrated in lower-paying sectors and informal employment, facing barriers to accessing high-paying and leadership roles.
Political Underrepresentation: Low representation of women in decision-making bodies such as parliament and state assemblies hinders legislative reforms and policies that could promote gender equity and address systemic barriers.
Way forward:
Gender Quotas: Implement and enforce quotas for women’s representation in parliament, state assemblies, and ministerial positions. This can be modelled after successful practices in other countries where gender quotas have significantly increased women’s political participation.
Equal Pay Initiatives: Enforce equal pay for equal work through rigorous monitoring and enforcement mechanisms. Encourage transparency in salary structures and promote awareness among employers and employees.
Mains PYQ:
Q Can the vicious cycle of gender inequality, poverty and malnutrition be broken through microfinancing of women SHGs? Explain with examples.(UPSC IAS/2021)
Persistent exclusion results in some disciplines becoming a last resort for many students with social sciences increasingly becoming a significant reservoir of the excluded in India.
Causes of Exclusion in Higher Education:
Excessive Competition: Premier institutions have stringent filtering mechanisms due to high demand, which results in significant exclusion of students.
Financial Factors: Private institutions often have high fees not regulated by statutory norms, and public institutions, facing reduced government funding, also increase fees, making education inaccessible for many.
Subject and Course Availability: There is a regional disparity in the availability of courses. Certain regions offer generic courses with outdated syllabi, limiting students’ choices and leading to exclusion.
Surge of Empirical Orientation:
Employability Perception: Courses with empirical and practical applications, like economics, are perceived to offer better employment opportunities compared to more theoretical courses like anthropology or sociology.
Policy Intervention Skills: There is a growing expectation for social science students to develop problem-solving skills similar to those of engineering students, which narrows the focus within social sciences.
Private Universities: The emergence of private universities catering to the affluent has led to a demand for courses that are less popular in public institutions, creating a dichotomy in course preference and quality.
Improving Quality of Higher Education:
Expand Quantity and Improve Quality: Increase the number of seats to accommodate excluded students and ensure concerted efforts towards enhancing the quality of education like entry based on competitive exams.
Enhance Teaching Quality: Prioritize the improvement of teaching methods and the content of courses to make education more relevant and effective for example reviewing and taking feedback on learning experiences from students.
Address Financial Exclusion: Implement measures to reduce financial barriers and prevent the widening of educational inequalities, ensuring that quality education is accessible to a broader demographic. For example, the Government can provide loans or scholarships.
Update Course Content: Regularly revise and update the syllabi to keep pace with societal changes and technological advancements, such as generative artificial intelligence.
Focus on Inclusivity: Ensure that policies and interventions in higher education focus on inclusivity, addressing the needs of diverse student populations and reducing regional disparities in course offerings.
Steps taken by Government
All India Council for Technical Education (AICTE) Initiatives: The AICTE has undertaken various initiatives to enhance the quality of technical education, such as the establishment of Deen Dayal Upadhyay KAUSHAL Kendras and the introduction of B.Voc degree programs.
University Grants Commission (UGC) Regulations: The UGC has notified regulations to improve the quality of higher education, including those related to recognition, accreditation, minimum qualifications for teachers, curbing ragging, and grievance redressal.
Scholarship and Fellowship Schemes: The UGC has launched various scholarship and fellowship schemes, such as the PG Doctoral Fellowship for SC/ST students, to promote inclusion and equity in higher education.
Conclusion: Efforts to enhance higher education, including expanding access, improving quality, and addressing financial barriers, are crucial for fostering inclusivity and equipping students for India’s future.
Mains PYQ:
Q The quality of higher education in India requires major improvement to make it internationally competitive. Do you think that the entry of foreign educational institutions would help improve the quality of technical and higher education in the country Discuss. (UPSC IAS/2015)
The king and queen of the “Onge tribe” welcomed a baby boy in the Andaman Islands, marking a significant moment for the tribe. With the arrival of the newborn, the tribe’s total population now stands at 136, as confirmed by an official source.
About Onge Tribe
The Onge are PVTGs (Particularly Vulnerable Tribal Groups) native to the Andaman Islands.
They have traditionally been hunter-gatherers and fishers, while also practising cultivation.
Their population significantly decreased after colonization, from 672 in 1901 to around 100.
They practice a form of animism, with ancestor worship being significant.
They traditionally make decisions through group consensus.
Today, the surviving members are confined to two reserve camps on Little Andaman: Dugong Creek in the northeast, and South Bay.
Genetically, the Onge are distantly related to East Asian populations and show affinities with Southeast Asian Negrito ethnic groups.
Other Indigenous People of Andaman and Nicobar
1. Great Andamanese Tribe
One of the largest tribes, the Great Andamanese tribe is currently settled on the Strait Island under the Andaman & Nicobar Administration. Despite their historic bravery, diseases and other challenges have reduced their population to 43 individuals as of the 2001 census.
Government initiatives: The administration provides housing, coconut plantations, and rationing to support their livelihoods and well-being.
2. Jarwas Tribe
Jarwas inhabit the Western coast of the Middle and South Andaman Islands. They are known to be hostile but have shown receptivity to friendly contact expeditions since 1974. Their present numbers are estimated at between 250–400 individuals.
Jarwas are nomadic hunters and gatherers, using traditional methods like bows and arrows for hunting and fishing.
3. Sentinelese Tribe
Sentinelese reside on the small North Sentinel Island, maintaining a wary stance towards outsiders.
Despite initial scepticism, contact expeditions have made progress since 1991, albeit with caution.
Who are the Particularly Vulnerable Tribal Groups (PVTGs)?
These groups are among the most vulnerable sections of our society as they are few in number, and have not attained any significant level of social and economic development.
They generally inhabit remote localities having poor infrastructure and administrative support.
75 such groups have been identified and categorized as Particularly Vulnerable Tribal Groups (PVTGs).
Origin of the concept
The Dhebar Commission (1960-1961) stated that within Scheduled Tribes there existed an inequality in the rate of development.
During the fourth Five Year Plan (1969-74) a sub-category was created within Scheduled Tribes to identify groups that were considered to be at a lower level of development.
This sub-category was named “Primitive tribal group”.
In 2006 the government of India proposed to renamePVTGs.
Features of PVTGs
The features of such a group include a:
Pre-agricultural system of existence
The practice of hunting and gathering
Zero or negative population growth
Extremely low level of literacy in comparison with other tribal groups
Groups that satisfied any one of the criteria were considered PTG.
PYQ:
[2019] Consider the following statements about Particularly Vulnerable Tribal Groups (PVTGs) in India:
PVTGs reside in 18 States and one Union Territory.
A stagnant or declining population is one of the criteria for determining PVTG status.
There are 95 PVTGs officially notified in the country so far.
Irular and Konda Reddi tribes are included in the list of PVTGs.
Q The public health system has limitations in providing universal health coverage. Do you think that the private sector can help in bridging the gap? What other viable alternatives do you suggest? (UPSC IAS/2015)
Q In order to enhance the prospects of social development, sound and adequate health care policies are needed particularly in the fields of geriatric and maternal health care. Discuss. (UPSC IAS/2020)
Mentors comment: In the last week of May, a tragic fire at a private neonatal care nursing home in New Delhi shocked everyone. Political parties started blaming each other, and the media exaggerated by incorrectly claiming that many nursing homes in Delhi operate without a license. Despite the intense media coverage, the incident has been largely forgotten, leaving the grieving parents behind. Instead of focusing on who to blame, it’s important to recognize that such tragedies are usually the result of systemic failures—in this case, the failure of health-care regulations.
Let’s learn–
Why in the news?
Health regulations are crucial, but their implementation in India needs to be thoughtful and carefully balanced.
Regulation and standards in the Indian health care system
Excessive and Complex Regulations: Some states have over 50 approvals required under multiple regulations for each healthcare facility, creating a bureaucratic burden. Despite the complexity, there is a perception among officials that the private health sector is under-regulated.
Unrealistic Standards: Many healthcare quality standards set by the government, such as those in the Clinical Establishments (Registration and Regulation) Act, 2010, and the Indian Public Health Standards (IPHS), are considered unrealistic and difficult to implement. Only a small percentage of government primary healthcare facilities meet these standards despite their aspirational goals.
Mixed health-care system in India
Diverse Healthcare Providers: India’s healthcare system includes both government and private sector providers, ranging from single-doctor clinics and small nursing homes to large corporate hospitals, each serving different population segments.
Dominance of Private Sector: The private sector delivers approximately 70% of outpatient services and 50% of inpatient services, indicating a significant reliance on private facilities for health care by the Indian population.
Regulatory and Quality Challenges: There are disparities in regulation enforcement and quality standards between the private and government sectors, with issues such as approval delays, cost of compliance, and ensuring consistent quality care across diverse facilities.
Challenges related to mixed health-care system
Regulatory Disparities: Uneven enforcement of regulations between private and government health facilities. Overzealous regulation of private facilities while government facilities face fewer consequences for similar infractions.
Approval Delays: Sluggish approval processes for private facilities, causing operational delays and financial strain. Long waiting periods for renewal applications, even when submitted well in advance.
Cost and Accessibility: High cost of services in large corporate hospitals compared to smaller clinics and nursing homes. Limited accessibility of government facilities for certain populations, despite being free or low-cost.
Differential Standards: Impractical to hold small clinics and nursing homes to the same standards as large hospitals. Need for a tiered approach to regulation, with essential and desirable standards based on facility type.
Financial Burden: High cost of compliance with regulations for smaller facilities, potentially making health services unaffordable for patients. The a need for government subsidies or funding to help smaller providers meet regulatory standards without increasing costs for patients.
Stakeholder Involvement: Insufficient involvement of health-care providers, facility owners, and community members in the formulation of regulations. Lack of representation from various types of facilities in regulatory processes.
Public Perception and Trust: Political rhetoric and sensational media coverage undermining trust in health-care providers. Potential for increased violence against health-care providers due to public mistrust.
Infrastructure and Safety: Inconsistent emphasis on essential safety measures like fire safety across facilities. Need for equitable implementation of safety standards in all healthcare buildings.
Affordable care is one need
Role of Small Providers: Single doctor clinics and small nursing homes are crucial for providing initial access and health services, particularly for middle-income and low-income populations. These smaller providers deliver a significant portion of health services at a lower cost compared to large corporate hospitals.
Supportive Regulations: There is a need for regulations that support small providers to keep healthcare costs low and affordable. Guidelines should be practical and implementable, harmonizing multiple regulations and simplifying the application process with timely approval.
Differential Approach: Regulations should recognize the different capabilities of various health facilities. Smaller clinics and nursing homes should not be held to the same standards as large hospitals to avoid escalating costs that could be transferred to patients. Essential and desirable regulatory points should be established, with regular self-assessments and inspections to ensure compliance.
Government subsidies and funding should be considered to help smaller facilities adhere to necessary regulations without increasing costs for patients.
Why do we need to Focus on the primary caregivers?
Accessibility and Affordability: Single-doctor clinics and small nursing homes provide essential health services at a lower cost, making health care more accessible and affordable for middle-income and low-income populations.
Primary Care Foundation: Promoting primary care helps manage health issues early, reducing the burden on secondary and tertiary care facilities and supporting the goals of the National Health Policy, 2017, for people-centric, accessible, and affordable health services.
Sustainable Support: Simplified, fair, and collaborative regulatory processes, along with government subsidies, can help primary-care providers operate effectively, ensuring quality and safety without escalating costs for patients.
Conclusion: Primary health care is crucial for achieving the SDG goal of universal health coverage by providing accessible, affordable, and quality health services, thus reducing the burden on higher-level care facilities and promoting overall health equity.
Q Public health system has limitations in providing universal health coverage. Do you think that the private sector can help in bridging the gap? What other viable alternatives do you suggest? (UPSC IAS/2015)
Q The increase in life expectancy in the country has led to newer health challenges in the community. What are those challenges and what steps need to be taken to meet them? (UPSC IAS/2022)
Mentor Comment: Health insurance, now central to India’s UHC policy, is being enhanced by digital advancements, enabling reforms akin to the U.S. but with cost-effective local adaptations. A South Indian healthcare chain recently integrated insurance and care provision, forming an Indian-style MCO. This prompts reflection on MCOs’ potential to extend universal health care in India significantly.
Let’s learn_ _
Why in the news?
Universal healthcare poses a multifaceted challenge, yet managed care organizations may offer a piece of the solution that Indian healthcare requires.
What is a Managed Care Organization?
A Managed Care Organization (MCO) is a health care company or a health plan that is focused on managed care as a model to limit costs, while keeping quality of care high.
The background of Managed Care Organizations (MCOs) in the United States and India:
Evolution of MCOs in the United States:
MCOs have their origins in rudimentary prepaid healthcare practices in the 20th century.
The mainstreaming of MCOs gained momentum in the 1970s due to concerns over healthcare costs.The economic slowdown post-1970s made high insurance premiums less attractive to purchasers.
A shift occurred towards integrating insurance and healthcare provisioning functions. Focus areas included prevention, early management, and cost control, all under a fixed premium paid by enrollees.
MCOs have evolved through multiple generations and forms, deeply penetrating the health insurance market. While evidence of their effectiveness in improving health outcomes and prioritizing preventive care is mixed, they have been effective in reducing costly hospitalizations and associated costs.
Evolution of MCOs in India:
The first public commercial health insurance emerged in the 1980s.The focus has primarily been on indemnity insurance and covering hospitalization costs.
There is a significant market for outpatient consultations, valued at nearly $26 billion.
Health insurance in India has traditionally lagged behind life and general insurance. The sector faces issues such as lack of innovation and high, often unsustainable, operational costs.
As per Thomas (2011), Health insurance has played a secondary role to other forms of insurance. The industry’s operational inefficiencies and high costs have been persistent issues.
Challenges in India:
Lack of Natural Incentives for Cost Control: The evolutionary trajectory of Indian health insurance has not incentivized consumer-driven cost control.
Target Demographic: Health insurance has mainly targeted a thin, urban, well-off segment, neglecting broader demographics.
Informality in Outpatient Practices: There is widespread informality among outpatient practices, complicating efforts to standardize and regulate care.
Lack of Clinical Protocols: The absence of widely accepted clinical protocols hampers the quality and consistency of care.
Economic Viability: Unprofitable operations and unaffordable premiums pose significant economic challenges, preventing sustainable growth and systemic improvement.
Limited Impact on UHC: Private initiatives, despite their potential, are unlikely to significantly contribute to Universal Health Coverage (UHC) without public support.
Insufficient Control Over Patient Journeys: Health insurers have little control over the patient’s journey before hospitalization, limiting their ability to manage early interventions and reduce costs through comprehensive outpatient care.
Prospective Solutions and Remaining Issues:
Potential for Big Healthcare Brands: Large healthcare brands with loyal urban patient bases and substantial resources may initiate successful managed care projects.
Need for Public Patronage: Exploring managed care with cautious and incremental public patronage could be promising, indicating a need for government involvement to achieve broader impacts.
Underutilization of Outpatient Insurance: Given the low share of insurance in outpatient care spending and the average of three consultations per year per person, there is significant potential to reduce healthcare costs through early interventions and comprehensive outpatient care coverage.
NITI Aayog Report:
Outpatient care insurance scheme: In 2021, NITI Aayog released a report advocating for an outpatient care insurance scheme based on a subscription model to enhance savings through improved care integration.
Yield significant benefits: A well-functioning managed care system can yield significant benefits, including consolidating practices, streamlining management protocols, and emphasizing preventive care in the private sector.
Catering for the beneficiaries of PMJAY: The report highlights the potential of incentives under the Ayushman Bharat Mission to encourage the establishment of hospitals in underserved areas catering to beneficiaries of the Pradhan Mantri Jan Arogya Yojana (PMJAY).
Conclusion: While Managed Care Organizations are not a perfect solution, they can play a role in addressing the complexities of achieving Universal Health Coverage (UHC) in India by being part of a broader strategy.
Over 30 years, a study examining 20 diseases revealed minimal advancements in narrowing the disparity between genders as per “the Lancet Public Health Journal”.
What does the New Lancet report say?
On Health Disparities: The study highlights that women tend to suffer more from lower back pain, depression, and headaches, while men have shorter life expectancies due to higher rates of road accidents, cardiovascular diseases, and, recently, COVID-19.
On Health Burden: Women spend more time in poor health, while men are more likely to die prematurely from severe conditions.
Overall Global Analysis: The analysis examines differences in the 20 leading causes of illness and death globally, considering all ages and regions.
What Causes the Differences in Diseases Between Women and Men? (Observations)
Biological Factors:
Hormonal Differences: Hormonal fluctuations in women, such as during menstrual cycles, pregnancy, and menopause, can influence susceptibility to certain conditions like migraines, depression, and autoimmune diseases.
Genetic Variations: Variations in genes and genetic predispositions may contribute to differences in disease susceptibility and severity between sexes.
Anatomical Variances: Physiological differences, such as in skeletal structure and hormonal regulation, can affect the manifestation of certain diseases like lower back pain and reproductive disorders.
Societal and Gender Norms:
Healthcare-Seeking: Societal norms and gender roles may influence healthcare-seeking behaviors, with men often less likely to seek medical attention for mental health issues due to perceived notions of masculinity.
Occupational Hazards: Occupational differences between genders can lead to varying exposures to health risks, with certain professions associated with higher rates of injury or exposure to harmful substances.
Socioeconomic Factors: Disparities in socioeconomic status can impact disease prevalence and outcomes differently for women and men.
Healthcare System Bias:
Diagnostic Bias: Gender biases in healthcare may result in underdiagnosis or misdiagnosis of certain conditions in women, leading to delays in treatment and poorer health outcomes.
Treatment Disparities: Differences in treatment approaches and responses may exist between sexes, with women sometimes receiving less aggressive treatment for cardiovascular diseases or being undertreated for pain conditions.
Research Bias: Historically, medical research has often focused on male subjects, leading to a lack of understanding of how diseases manifest and progress differently in women.
No Improvement in Care for Women Over Time
Stable Gender Gap: Despite overall health improvements, the disparity between male and female health conditions remains stable.
Conditions Affecting Women: Conditions like lower back pain and depressive disorders have shown little to no decrease over time compared to male-dominated conditions.
Reproductive Focus: Global health systems have historically focused on women’s reproductive health, neglecting other significant health issues affecting women.
What Needs to Be Done (Way Forward)
Better Data Collection: Governments should consistently collect and categorize health data by sex and gender to better understand and address health disparities.
Targeted Health Interventions: Specific health interventions should be developed and implemented based on detailed sex and gender data.
Increased Funding: More financial resources should be allocated to underfunded conditions that disproportionately affect women, such as mental health.
Addressing Healthcare Bias: Efforts should be made to eliminate biases in healthcare to ensure women receive appropriate and timely treatment for their conditions.
Mains PYQ:
Q Can the vicious cycle of gender inequality, poverty and malnutrition be broken through microfinancing of women SHGs? Explain with examples. (UPSC IAS/2021)
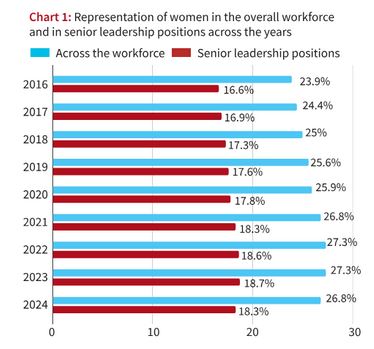
Although women’s representation in the workforce has grown over the years “LinkedIn’s Economic Graph data” indicates that progress has stalled since 2022 and declined in 2024.
What does the data show?
Representation of women in the workforce has increased over the years but progress has stalled since 2022 and declined in 2024. The promotion of women to senior and leadership roles has stagnated in recent years.
Sectors like healthcare, education, administrative, and support services have higher female representation in senior positions, while sectors like manufacturing, construction, oil, and gas have poor representation.
Representation of women in the overall workforce and in senior positions
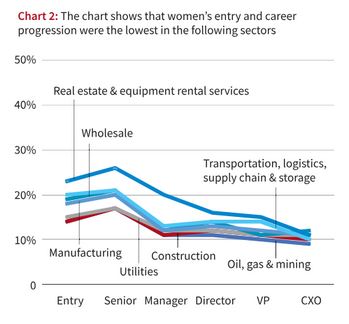
Entry and career progression of women
Oil, Gas, and Mining: Among the lowest representation of women in leadership roles, at around 11%.
Construction: Very few women are represented, especially in senior roles.
Utilities: Women face significant barriers in advancing to leadership positions.
Wholesale: Low entry and career progression for women.
Manufacturing: Poor representation of women across all positions, including senior roles.
Transportation: Limited career progression opportunities for women.
Real Estate: Few women in leadership positions, with significant entry barriers.
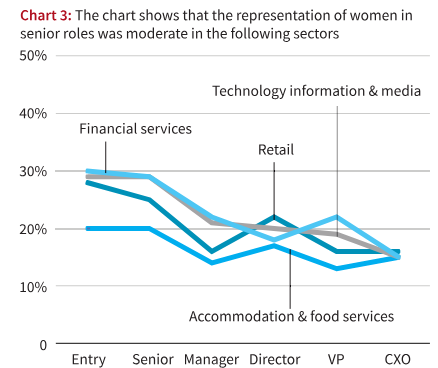
About the accommodation and other services
Representation of women in senior roles within the accommodation and food services sector falls between 15% and 20%.
This sector exhibits a moderate level of female representation compared to other industries.
While not the highest, it surpasses sectors like oil, gas, mining, construction, utilities, wholesale, manufacturing, transportation, and real estate, where women hold just 11%-14% of leadership positions.
The data suggests there’s still room for improvement in increasing the number of women in leadership roles within the accommodation and food services sector.
Efforts to improve gender diversity and inclusion should be continued and perhaps intensified in this sector, aligning with broader industry and societal goals for gender parity in the workforce.
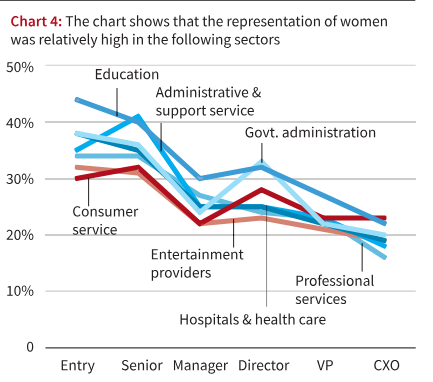
Administrative and support services:
Women hold senior positions in administrative and support services at a rate of 22% to 30%, indicating a moderate level of representation compared to other sectors.
This sector demonstrates a higher level of female representation in leadership roles compared to industries like oil, gas, mining, construction, utilities, wholesale, manufacturing, transportation, and real estate, where women’s leadership roles range from 11% to 14%.
The education sector boasts the highest representation of women in senior positions at 30%, suggesting that sectors like administrative and support services still have room for improvement.
Efforts to promote gender diversity and inclusion within administrative and support services should be sustained, aiming for further increases in the representation of women in leadership roles.
Continued focus on addressing biases, societal norms, and structural barriers is essential to achieving greater gender parity and advancement opportunities for women within this sector.
Way Forward
Efforts by policymakers and business leaders are needed to tackle challenges faced by women in reaching leadership roles, focusing on “women-led development”.
Stricter enforcement of laws such as the Companies Act, 2013, which mandates women directors on company boards. Between April 2018 and December 2023, 507 companies were fined for non-compliance, with 90% being listed companies.
Mains PYQ
Q Micro-Finance as an anti-poverty vaccine, is aimed at asset creation and income security of the rural poor in India”. Evaluate the role of the Self Help Groups in achieving the twin objectives of empowering women in rural India. (UPSC IAS/2020)
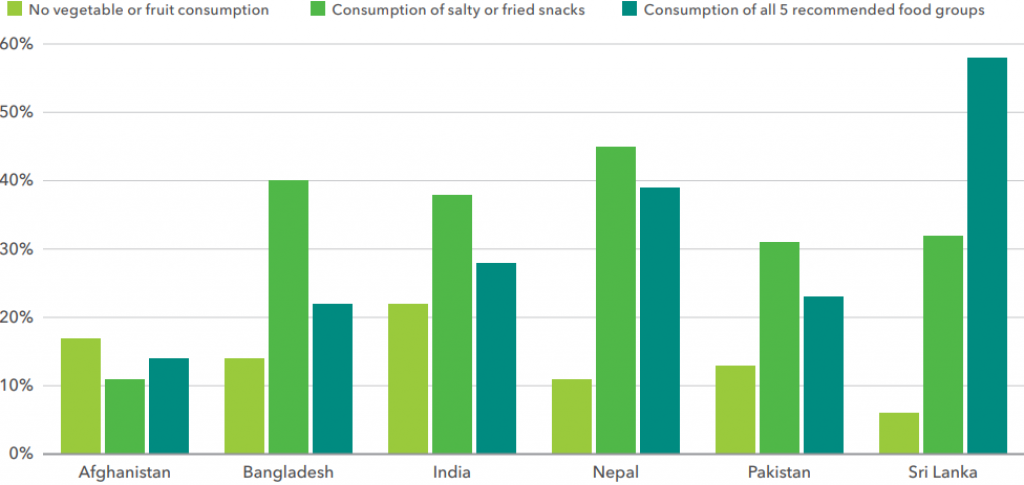
A global report highlights a significant rise in unhealthy food consumption in India, surpassing intake of vegetables, fruits, and other nutritious foods.
Global Food Policy Report 2024: Food Systems for Healthy Diets and Nutrition was released by “theInternational Food Policy Research Institute (IFPRI)”.
About CGIAR:
CGIAR (formerly the Consultative Group on International Agricultural Research) is a global partnership uniting organizations engaged in research for a food-secure future.
Focus: Its mission focuses on reducing poverty, enhancing food and nutrition security, and improving natural resources and ecosystem services.CGIAR conducts research and partners with other organizations to transform global food systems and ensure equitable access to sustainable, healthy diets.
Emerging Trends in India:
Increase in consumption of unhealthy food: There is a significant increase in the consumption of unhealthy foods such as salty or fried snacks compared to nutritious options like vegetables and fruits. About 38% of the population consumes unhealthy foods, while only 28% consume all five recommended food groups.
The consumption of processed foods and ready-made convenience foods is rising. From 2011 to 2021, malnutrition in India increased from 15.4% to 16.6%.The prevalence of overweight adults rose from 12.9% in 2006 to 16.4% in 2016.
Processed food consumption is on the rise in India
South Asian Highlights
Processed Food Consumption: Increasing intake of processed foods like chocolates, salty snacks, beverages, and ready-made meals in India and other South Asian countries.
Malnutrition Rates: High levels of undernutrition and micronutrient deficiencies coexist with rising rates of overweight, obesity, and diet-related noncommunicable diseases (NCDs).
Food Budget Trends: Packaged food spending in India’s household food budgets nearly doubled from 6.5% to 12% between 2015 and 2019.
Issue of Double Malnutrition:
Double malnutrition refers to the coexistence of undernutrition and micronutrient deficiencies with overweight and obesity, or diet-related noncommunicable diseases (NCDs).
High levels of undernutrition (stunting and wasting) and micronutrient deficiencies persist even as overweight and obesity rates increase.
More than two billion people, especially in Africa and South Asia, cannot afford a healthy diet.
Dietary Guidelines by ICMR:
The Indian Council of Medical Research (ICMR) released 17 dietary guidelines to promote healthy eating.
Guidelines emphasize reading food labels to make informed choices and minimizing the consumption of high-fat, sugar, salt, and ultra-processed foods.
The guidelines highlight the importance of diverse diets over cereal-centric agriculture and food policies.
ICMR advises against the misleading information often presented on packaged foods.
Way forward:
Strengthen Nutritional Policies: Develop and enforce policies that promote the consumption of nutritious foods. Implement taxes on unhealthy foods and subsidies for fruits, vegetables, and other micronutrient-rich foods.
Regulate Processed Foods: Implement strict regulations on the marketing of unhealthy foods, especially targeting children.
Mains PYQ:
Q How far do you agree with the view that the focus on the lack of availability of food as the main cause of hunger takes the attention away from ineffective human development policies in India? (15) (UPSC IAS/2018)
The ECI’s election announcement lacked sign language interpreters, highlighting the everyday exclusion of Deaf and Hard of Hearing (DHH) citizens.
Present Issue:
India’s societal and structural framework often neglects the needs of Deaf and Hard of Hearing (DHH) citizens.
This exclusion is evident in various aspects of daily life, such as the absence of sign language interpreters during major public announcements and inadequate accessibility in public services.
Sign Language versus Oralism
The Indian education system predominantly employs “oralism,” which emphasizes teaching deaf individuals to use their voices and lip-read, rather than using sign language.
This approach has been criticized for perpetuating social isolation and failing to remove barriers that hinder the integration of DHH individuals.
In contrast, using sign language has been shown to aid cognitive development and prevent linguistic deprivation.
Over 70 countries recognize their national sign languages legally, promoting accessibility and inclusion for deaf citizens.
Present Scenario:
As per WHO estimates in India, there are approximately 63 million people, who are suffering from Significant Auditory Impairment; this places the estimated prevalence at 6.3% in the Indian population.
As per the NSSO survey, currently, 291 persons per one lakh population are suffering from severe to profound hearing loss (NSSO, 2001).
Of these, a large percentage are children between the ages of 0 to 14 years.
What Does the 2011 Census Say?
The 2011 Census reported five million hearing-impaired individuals in India, while the National Association of the Deaf estimates 18 million.
Despite these large numbers, DHH individuals are often excluded from educational and employment opportunities. Only 5% of deaf children attend school, and they face prolonged graduation timelines due to oralist-focused curricula.
Government initiatives for employing the deaf are often ineffective, and there is a lack of ISL recognition, despite repeated demands and protests.
The National Programme for Prevention and Control of Deafness
The program was initiated in the year 2007 in pilot mode in 25 districts of 11 States/UTs. It has been expanded to other districts too after the 12th five-year plan.
The Program was a 100% Centrally SponsoredScheme during the 11th Five-year plan. However, as per the 12th Five Year Plan, the Centre and the States will have to pool in resources financial norms of NHRM.
However, it falls short of addressing the quality of life for DHH individuals. This program has been expanded to 228 districts of 27 States / U.Ts in a phased manner.
Objectives of the program:
To prevent avoidable hearing loss on account of disease or injury.
Early identification, diagnosis, and treatment of ear problems responsible for hearing loss and deafness.
To medically rehabilitate persons of all age groups, suffering from deafness.
To develop institutional capacity for ear care services by providing support for equipment and material and training personnel.
Components of the Programme:
Manpower Training & Development to grassroots level workers.
Service Provision Including Rehabilitation – Screening camps for early detection of hearing impairment and deafness.
Awareness Generation for early identification of the hearing impaired.
Monitoring and Evaluation.
What Needs to be done?
Official Recognition of ISL: ISL should be recognized as an official language, and its use should be integrated into educational systems and public services. Teaching ISL in schools, colleges, and to the general public will promote inclusivity and fluency.
Inclusive Health Care: Health care systems need to be updated to ensure accessible communication for DHH patients. This includes training more ISL interpreters and reducing barriers for DHH individuals pursuing healthcare professions.
Media and Public Communication: Media channels should incorporate ISL interpretation and subtitles, especially in Hindi and regional languages. Government event announcements should have live ISL interpreters to ensure accessibility.
Employment Opportunities: Creating more employment opportunities for DHH individuals, beyond low-skilled jobs, is essential. This includes training and employing DHH individuals as ISL instructors and ensuring accessible workplaces.
Conclusion: To ensure inclusivity for DHH citizens, India must officially recognise ISL, integrate it into education and public services, improve healthcare accessibility, and expand employment opportunities and mental health support.
Mains PYQ:
Q How have digital initiatives in India contributed to the functioning of the education system in the country? Elaborate your answer. (UPSC IAS/2020)
Mains: Q What are the continued challenges for Women in India against time and space? (UPSC IAS/2019)
Q. Discuss the positive and negative effects of globalization on women in India. (UPSC IAS/2015)
Prelims:
Which of the following statements is/are correct regarding the Maternity Benefit (Amendment) Act, 2017? (UPSC IAS/2019)
1. Pregnant women are entitled for three months pre-delivery and three months post-delivery paid leave. 2. Enterprises with crèches must allow the mother minimum six crèche visits daily. 3. Women with two children get reduced entitlements.
Select the correct answer using the codes given below: (a) 1 and 2 only (b) 2 only (c) 3 only (d) 1, 2 and 3
Note4Students:
Prelims: POCSO Act; Medical Termination of Pregnancy (MTP);
Mains: Society; Women Issues;
Mentor comment: Did you know that there are around 1,49,404 total cases of crimes against children, with varying rates across states and union territories? Within this, Sexual crimes are prevalent with a high number of offenses against girls compared to boys. Hence, the Protection of Children from Sexual Offences Act (POCSO) was passed in 2012 to comprehensively deal with the issue of sexual offenses against children. POCSO not only spells out the punishments for offenses but also sets out a system for support of victims and improved methods for catching offenders. Recently, this issue has been contentious, citing the importance of maintaining consistency within the laws and legislation availed by the Indian Government.
Let’s learn.
–
Why in the News?
The “Scheme for Care and Support to Victims under Sections 4 & 6 of the Protection of Children from Sexual Offences (POCSO) Act, 2012” which was introduced by the Ministry of WCD has faced criticism for its lack of clarity, inconsistencies, and failure to align with existing legislation.
About the Scheme for Care and Support to Victims of the POCSO Act, 2012:
It is a centrally funded initiative from the NIRBHAYA fund of the Ministry of Women and Child Development.
The scheme seeks to address the challenges faced by minor pregnant girl victims and fill the gaps in existing support systems. It aims to provide integrated support services for emergency and long-term rehabilitation.
Sections 4 & 6: The services provided under this include a comprehensive range of support and assistance for minor pregnant girl victims who have experienced sexual assault or abuse.These services aim to address the challenges faced by these victims and ensure their well-being and rehabilitation.
What are the issues surrounding this Scheme?
Inconsistencies with Legislation:
Incorrect interpretation of Section 27 of the POCSO Act, 2012, regarding medical examination of minors. There is some misrepresentation of the Child Welfare Committee’s authority regarding sexual assault medical examination.
Delaying stipulation in the Medical Termination of Pregnancy (MTP) process contradicts the MTP Act. There are limited references to MTP options within the scheme.
Expanded Scope Without Corresponding Revisions: The scheme initially targeted abandoned or orphaned pregnant girls, and now includes all pregnant girl victims under the POCSO Act. This kind of lack of proper redrafting to reflect inclusiveness results in confusion.
Adolescent Sexual Health Education and Prevention: The scheme has failed to address adolescent sexual health needs and perpetuates a reactive approach to sexual violence. There is a need for proactive Sexual and Reproductive Health (SRH) information and services for youth.
Empirical data suggests cases of pregnancy due to consensual relationships, highlighting the importance of comprehensive SRH education.
Monetary Implications: Proposed financial support includes an initial payment of ₹6,000 and a monthly payment of ₹4,000 until age 21, extendable to 23. Hence, due to the high incidence of child marriages and teenage pregnancies, there is an increased financial burden.
Contrary to Rules and Regulations: The Pregnant victims under the POCSO Act are not automatically classified as Children in Need of Care and Protection (CNCP). The Scheme mandates treating all pregnant girls as CNCP, contrary to POCSO Rules and the Juvenile Justice Act.
Therefore, the unnecessary procedural burdens are imposed on victims due to misclassification
Way Forward:
Streamlined Procedures: Govt. needs to simplify the application and support process to make it more accessible to POCSO victims.
Enhanced Outreach: India needs to increase its awareness through targeted campaigns and partnerships with civil societies and community organizations.
Technology Integration: For timely delivery and efficient implementation, the utilization of technology is necessary to streamline services and provide easier access to support.
Training and Capacity Building: Invest in training for staff and volunteers to enhance service delivery.
[2022] The increase in life expectancy in the country has led to newer health challenges in the community. What are those challenges and what steps need to be taken to meet them?
[2020] Critically examine the role of WHO in providing global health security during the Covid-19 pandemic.
Note4Students:
Prelims: NA
Mains: Hypertension, WHO’s HEARTS Strategy, India’s Hypertension Control Initiative (IHCI)
Mentor’s Comment: Hypertension, a major but overlooked risk factor for heart attacks and strokes, causes 10.8 million preventable deaths annually, surpassing risks like tobacco use and high blood sugar. The WHO’s 2023 report reveals that 1.3 billion adults globally have hypertension, with 46% unaware of their condition. In India, 311 million adults suffer from hypertension, triple the number with diabetes.
Let’s learn___
Why in the News?
Over the past three years, the COVID-19 vaccine has attracted significant public attention as a potential risk factor for blood clot formation, leading to sudden cardiac arrest.
What is Hypertension?
Hypertension (high blood pressure) is when the pressure in your blood vessels is too high (140/90 mmHg or higher). It is common but can be serious if not treated. Eating a healthier diet with less salt, exercising regularly and taking medication can help lower blood pressure.
WHO Report on Hypertension
2023 WHO Report: In 2023, the World Health Organization (WHO) released its first-ever report on hypertension titled “Global Report on Hypertension: The Race against a Silent Killer.”
Silent Killer: Hypertension is often called a silent killer because people are usually unaware of their high blood pressure until they develop complications.
Leading Cause of Death: High blood pressure causes more deaths than other leading risk factors, such as tobacco use and high blood sugar.
Rising Numbers: The number of adults with hypertension nearly doubled since 1990 to reach 1.3 billion.
Awareness and Control: Globally, an estimated 46% of adults with hypertension are unaware of their condition, and less than half (42%) are diagnosed and treated. Only one in five adults (21%) with hypertension has it under control.
Hypertension in India
Prevalence in India: The Indian Council of Medical Research-INdia DIABetes (ICMR-INDIAB) study estimates that in India, 311 million people (or one in every three adults) have hypertension.
Comparison with Diabetes: In India, adults with hypertension are threefold of the estimated 101 million people living with diabetes.
Dietary Salt and Hypertension
Impact of Excess Salt: Excess dietary salt intake (five grams or more per day) is a key risk factor for hypertension and contributed to two million cardiovascular disease deaths in 2019.
Benefits of Reducing Salt Intake: Research shows that reducing salt intake can reduce cardiovascular disease risks by 30% and mortality by 20%.
Salt Consumption in India: Indian adults consume on average eight to 11 grams of salt per day, which is approximately twice the WHO-recommended daily intake.
Deaths Due to High Salt Intake: High salt intake is responsible for an estimated 175,000 deaths in India.
Hypertension across Socio-Economic Groups
Universal Impact: Hypertension affects all socio-economic groups.
Health Camps Findings: A Delhi-based NGO, Foundation for People-centric Health Systems, conducted 50 health camps in five localities of Delhi and Gurugram from October 2023 to March 2024, screening and treating around 12,000 people.
Detection in Low-Income Groups: Many were women, migrant workers, and rickshaws and taxi drivers from low-income groups. A large number were found to have diabetes and hypertension, with most cases detected for the first time in these camps, indicating gaps in awareness, detection, and treatment.
Back2Basics: India’s Hypertension Control Initiative (2021):
Objective: India aims to put 75 million people with hypertension and/or diabetes on standard care by 2025.
Initiation and Expansion: The IHCI, a collaborative project of ICMR, Ministry of Health and Family Welfare/Directorate General of Health Services, WHO India, and other partners, was initiated in November 2017 in 25 districts across five states and expanded to 140-plus districts of India in 2023.
Strategies: IHCI follows five simple and scalable strategies implemented through primary health care:
-Simplified drug and dose-specific treatment protocols for primary-care settings. -Strengthening the drug supply chain by including protocol-based drugs in the State essential drug list, forecasting drugs based on morbidity, and ensuring adequate budget allocation in annual plans. -Team-based and decentralized care. -Patient-centric measures such as dispensing 30 days of medicine during each patient visit. -Use of information systems for program monitoring.
Programmatic Learnings from IHCI
Access and Utilization: Nearly six years of IHCI implementation has resulted in two major learnings:
Simple treatment protocols with fewer drugs, reliable drug supply, linking patients to facilities closer to home for follow-up, and engaging teams increase access and utilization of health services from government facilities.
Simplified program monitoring makes performance assessment quantifiable and actionable.
Recognition: The IHCI won the 2022 UN Interagency Task Force and WHO Special Programme on Primary Health Care Award.
Future Goals and Prevention
Global Goals: Seventy-six million cardiovascular deaths and 450 million disability-adjusted life years (DALYs) could be avoided if countries achieve 50% population hypertension control by 2050.
India’s Targets: An estimated 4.6 million deaths can be prevented in India by 2040 if half the hypertensive population has its blood pressure under control, helping to achieve targets under the National Health Policy and global commitments like universal health coverage.
Way Forward
Raise Awareness: Educate the public about the risks and long-term adverse impacts of untreated hypertension. High blood pressure can affect multiple organs, including the heart, kidneys, brain, and eyes.
Scale Up Evidence-Based Interventions: Expand successful programs like IHCI. Use strategies and lessons from such experiences to design interventions for other lifestyle diseases like diabetes and chronic kidney diseases.
Focus on Non-Modifiable Risk Factors: Address non-modifiable risk factors such as family history, age over 65 years, and pre-existing comorbidities like diabetes and/or kidney disease. Focus on healthy adults with known non-modifiable risk factors.
Reduce Dietary Salt Consumption: Implement strategies like “SHAKE the salt habit” under WHO’s HEARTS strategy:
Surveillance to measure and monitor salt use.
Harness industry to promote and reformulate foods with less salt.
Adopt standard labelling and marketing.
Educate and communicate to empower individuals to eat less salt.
Support environments that promote healthy eating.
Conclusion: As hypertension continues to exact a heavy toll on global health, concerted efforts are needed to raise awareness, implement evidence-based interventions, and promote healthier lifestyles. By prioritizing hypertension control initiatives and fostering a culture of preventive healthcare, we can mitigate the devastating impact of this silent killer on communities worldwide.
Q Are tolerance, assimilation and pluralism the key elements in the making of an Indian form of secularism? Justify your answer. (UPSC IAS/2022)
Q How the Indian concept of secularism different from the western model of secularism? Discuss. (UPSC IAS/2018)
Q What are the challenges to our cultural practices in the name of Secularism? (UPSC IAS/2019)
Prelims:
Consider the following statements: (UPSC IAS/2020) 1. The Consititution of India defines its ‘basic structure’ in terms of federalism, secularism, fundamental rights and democracy. 2. The Constitution of India provides for ‘judical review to safeguard the citizens’ liberties and to preserve the ideals on which the Constitution is based. Which of the Statements given above is/are correct? (1) 1 only (b) 2 only (c) Both 1 and 2 (d) Neither 1 nor 2
Note4Students:
Prelims: Political Theories; Secularism
Mains: Society; Secularism;
Mentor comment: India since its Independence has been an observer of major democratic shifts, especially when it comes to the Political Parties. In the Indian kind of Parliamentary Democracy, the State is prohibited from patronizing any particular religion as the ‘State religion’ (positive secularism) and is enjoined to observe neutrality. The positive part of the Indian kind of Secularism is that it (the state) has been entrusted to regulate by Law (Procedure established by Law) or by an Executive order (head of govt.). In studies of Religion, the present modern democracies are generally recognized as secular. This is due to the near-complete freedom of religion (religious beliefs generally are not subject to legal or social sanctions), and the lack of authority of religious leaders over political decisions. However, in present Indian democratic politics, there exist two major binary contradictions – between the modern ‘secular subalterns’ (by R. Gandhi) vs. ‘Hindu subalterns’ (by PM Modi). This is for the first time that India is observing major shift in its Political Representation and the associated subalterns (subordinates).
Let’s learn
_
Why in the News?
The 2024 Indian General Election is being framed as a contest between “Subaltern Hindutva” and “Subaltern secularism”.
What is ‘Subaltern Secularism’?
The concept of “subaltern secularism” refers to the idea of secularism being embraced and practiced by marginalized or oppressed groups in society, often in contrast to the secularism associated with the elite classes or the classes that are in major power. Concerning ‘Secularism’, the “subaltern groups” are those who have been excluded from the dominant discourse on secularism, which has traditionally been associated with the English-speaking elite.
What is ‘Subaltern Hindutva’? : The “subaltern Hindutva” refers to a political strategy that mobilizes marginalized or subaltern Hindu groups by appealing to their sense of honor and identity within Hindu society. This concept emerged as a significant force in Indian politics, particularly since the 2014. Subaltern Hindutva gained traction by addressing the perceived contempt faced in the English-speaking elite circles, especially as more of them became educated.
Agenda of ‘Social Welfare’ set by‘Subaltern Secular’ Group:
On Reservation: They promised a dedicated ministry for the empowerment of the Other Backward Classes (OBC), the creation of a National Council for Social Justice, reservation in the higher judiciary for Scheduled Castes (SC), Scheduled Tribes (ST) and OBCs, and a Rohit Vemula Act for students of disadvantaged sections.
Political representation for weaker sections: Due to the lost regional subalterns in the post-Mandal era, they amended their constitution to reserve 50% of seats to the Congress Working Committee (CWC) for SCs, STs, OBCs, women, and minorities.
Legal guarantees for Minimum Income: They promised “Sampoorna Samajik Suraksha”, and a Nyuntam Aay Yojana (Nyay) as social security that will have legal guarantees for minimum income and social security for the poor.
Social and Health Security: Right to Health, pensions for Single Women, Elderly, and persons with disabilities, a Comprehensive Integrated Child Development Scheme in line with the National Food Security Act, and quality elementary schooling and maternity entitlements are promised.
How does the present ‘subaltern secularism’ differ from then ‘traditional secularism’?
By focusing on marginalized or oppressed groups: In ‘traditional secularism’, the discourse is often dominated by the elite, leading to a disconnect with the masses. On the other hand, ‘subaltern secularism’ challenges this top-down approach by advocating for the inclusion of marginalized voices in shaping secular narratives and practices
By practicing secular values: ‘Traditional secularism’ tends to be associated with the privileged classes and can sometimes overlook the perspectives of marginalized communities, ‘subaltern secularism’ seeks to empower these groups by providing them with a platform to express and practice their secular beliefs within their unique socio-political contexts.
What are the implications of ‘Subaltern secularism’ for Indian Democracy?
By focusing on marginalized or oppressed groups embracing and practicing secular values, subaltern secularism challenges the traditional elite-centric narrative of secularism in India.
Brings Inclusive Representation: It emphasizes the inclusion of diverse voices and perspectives in the secular discourse, ensuring that the concerns and experiences of marginalized communities are acknowledged and addressed within the democratic framework.
Empowering the Marginalized Groups: It can empower marginalized groups by providing them with a platform to express their secular beliefs and practices, enabling them to participate more actively in the democratic process and shaping the political landscape.
Counterbalancing the Dominant powers: By offering an alternative to dominant religious and social hierarchies, subaltern secularism can serve as a counterbalance to forces that seek to marginalize or oppress certain communities based on religious or social identities.
Challenges to Existing Power Structures: Subaltern secularism challenges existing power structures by advocating for a more inclusive and equitable society, where the rights and voices of all individuals, especially those from marginalized backgrounds, are respected and protected.
Political Strategy and Mobilization: Embracing subaltern secularism as a political strategy can help opposition parties like the Indian National Congress mobilize subaltern voters who have been historically marginalized, thereby reshaping electoral dynamics and promoting a more inclusive democracy.
Conclusion: For this strategy (social welfare) to succeed, the ‘secular subalterns’ will need to build robust political campaigns aligned to its new secular thinking, breaking away from its previous characteristic timidity.
On the occasion of World Immunisation Week observed from 24th to 30th April, the Indian Academy of Paediatricshas launched a campaign to focus on routine immunization as the ‘Birth Right’ of a Child.
About Measles Vaccination
This vaccine protects against 3 diseases: Measles, Mumps, and Rubella (MMR).
Centre for Disease Control and Prevention (CDC)recommends children get two doses of MMR vaccine, starting with the first dose at 12 -15 monthsof age, and the second dose at 4-6 years of age. Teens and adults should also be up to date on their MMR vaccination.
Indian Government Initiatives:
World Immunization Week: The Indian Academy of Paediatrics (IAP) launched a campaign during World Immunisation Week (April 24-30) focusing on routine immunization as a fundamental right of every child. IAP urged the government to expedite the introduction of the HPV vaccine and typhoid conjugate vaccine to address significant public health burdens.
Vaccination made within the country:
DTP Vaccine: 93% of surviving infants received the third dose of the DTP vaccine.
Measles Vaccine: 90% of infants received the second dose of the measles vaccine. The measles vaccine has been the most significant in reducing infant mortality, accounting for 60% of lives saved through immunisation since 1974.
Present issues include inequitable distribution of vaccines, inability to reach 90% coverage, human resource gaps, and financing problems. In 2022, 33 million children missed a measles vaccine dose, with 22 million missing the first dose and 11 million missing the second dose.
Impacts of Immunisation Globally:
Lives Saved: Immunisation efforts have saved an estimated 154 million lives globally over the past 50 years, equating to six lives every minute of every year.
Infant Mortality Reduction: 101 million of the lives saved were infants. Vaccination against 14 diseases has reduced infant deaths by 40% globally and by over 50% in Africa.
Diseases Targeted: Vaccines have contributed to reducing deaths from diseases like Diphtheria, Haemophilus Influenzae Type B, Hepatitis B, Japanese Encephalitis, Measles, Meningitis A, Pertussis, invasive Pneumococcal disease, Polio, Rotavirus, Rubella, Tetanus, Tuberculosis, and Yellow fever.
Conclusion: Immunisation saves lives, reduces infant mortality, and prevents outbreaks by protecting against infectious diseases, ensuring healthier communities, and securing a better future for children worldwide.
Mains PYQ:
Q What is the basic principle behind vaccine development? How do vaccines work? What approaches were adopted by the Indian vaccine manufacturers to produce COVID-19 vaccines? (UPSC IAS/2022)
Once again, the Muslim population has become a point of discussion. Last month, PM Narendra Modi referred Muslims in India, suggesting they have a higher birth rate.
Trends of Muslim Population as per Data Point (NFHS-5 2019-21) published on April 23:
Population Trends: The Economic Advisory Council to the Prime Minister noted a Muslims in the total population increased by 43.15% between 1950 and 2015, the share of Hindus decreased by 7.82% between 1950 and 2015.
The fertility rate of Muslims was 2.36 in 2019-21, much closer to the replacement level. The fertility rate is the average number of children a woman is expected to have in her lifetime. A rate of 2.1 (the ‘replacement level’) means that the population is stable.
Factors behind the High Population Growth of Muslims:
Socio-economic Factors: Socio-economic factors, rather than religion, significantly influence fertility rates. Educating girls, delaying marriage, promoting family planning awareness, and ensuring access to family planning measures are crucial in reducing fertility levels.
Regional Variations: Fertility rates among Muslim women vary regionally, influenced by the social and economic development of states.
Early Marriage and Literacy: There’s a positive correlation between higher fertility rates and early marriage among women aged 20-24. Conversely, a negative correlation exists between literacy rates among women and fertility rates.
Lack of Awareness: Lack of awareness about family planning remains a concern, with a significant portion of women reporting never hearing or seeing family planning messages.
Unmet Demand for Family Planning: Many women, particularly Muslims in certain states, have an unmet demand for family planning due to various factors, including lack of access to contraceptive measures.
Government Intervention: Increasing awareness about contraceptives, improving access to family planning measures, educating girls, and preventing child marriages are essential government functions to reduce fertility rates across religious groups.
Need for Coercive Measures:
Comprehensive Education and Awareness Programs: Implement educational campaigns that promote family planning, gender equality, and reproductive health awareness, targeting both men and women in communities across the country.
Access to Family Planning Services: Ensure easy access to a wide range of family planning methods and contraceptives, including in remote and underserved areas, through government health facilities and community outreach programs.
Mains PYQ:
Q Critically examine whether growing population is the cause of poverty OR poverty is the mains cause of population increase in India. (UPSC IAS/2015)

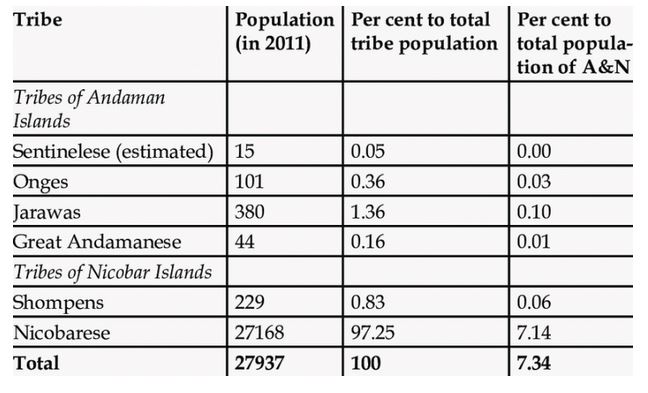
![[7th June 2024] The Hindu Op-ed: Health regulations need a base-to-top approach](https://dev.civilsdaily.com/wp-content/uploads/2024/06/7-June-2nd-1568x882.jpg)